
By Kumar Pillai

What does skin have to do with bones? Skin produces vitamin D that keeps the bones healthy. Exposure of skin to sunlight produces the sunshine hormone, vitamin D, that is required for proper absorption of calcium and phosphorous from the intestine, which is deposited in bones and keeps them strong and healthy. It is now known that vitamin D is important not only for bone health, but for the overall health of humans.
The Sun and Vitamin D
Vitamin D is unique because it can be synthezised in the skin exposure to sunlight. The precursor of vitamin D3, 7-dehydrocholesterol, is produced in relatively large quantities in the skin. 7-Dehydrocholesterol interacts with UVB light at wavelengths between 270 and 300 nm, with peak synthesis occurring between 295 and 297 nm.1 These wavelengths of electromagnetic radiation are present in sunlight, as well as in the light emitted by UV lamps in tanning beds, which produce UV light primarily in the UVA spectrum. Thus, vitamin D is not technically a vitamin, because vitamins are classified as compounds that our bodies cannot make and which we must obtain from our food. It is not just humans who produce vitamin D from sunlight. Vitamin D2 is produced from the UV irradiation of the yeast, sterol ergosterol, and is found naturally in sun-exposed mushrooms.2
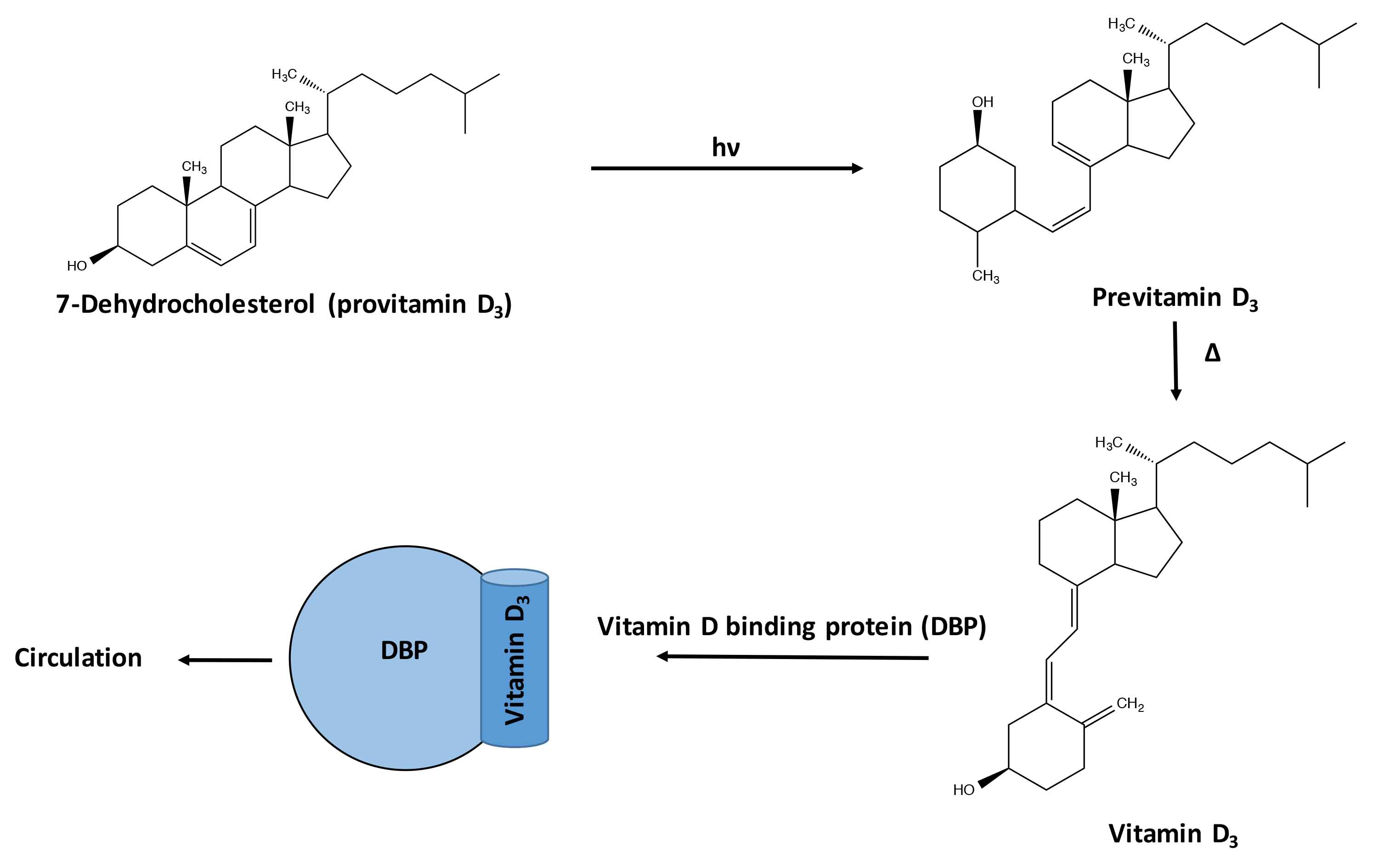
Figure 1: Schematic of the conversion of 7-dehydrocholesterol (provitamin D3) to vitamin D3 and its binding with vitamin D binding protein where it enters the blood stream.
The Role of Skin in Vitamin D Synthesis
Vitamin D3 that is produced in the skin is metabolized primarily in the liver to the major circulating form, 25-hydroxy vitamin D3 [25(OH)D3]. This molecule is metabolized in the kidney to produce the biologically active form of the hormone, 1,25-dihydroxy vitamin D3 [1,25(OH)2D3]. The skin not only participates in the production of vitamin D3, but also contains receptors for 1,25(OH)2D3, suggesting a role of this hormone in the growth and differentiation of this tissue.3 1,25(OH)2D3 appears to play a role in epidermopoiesis and melanin pigmentation.4 Not only is 1,25(OH)2D3 produced in keratinocytes, this hormone also regulates keratinocyte differentiation and modulates calcium induced epidermal differentiation.3 There is also evidence that different areas of human body have vastly different capacities to make vitamin D from sun.5 Vitamin D has also been claimed recently to prevent sunburn. It was found that a high dose of vitamin D attenuated the inflammatory response to UV radiation in a small group of normal volunteers.6
Human Evolution, Skin Color, and Vitamin D Status
The natural selection hypothesis suggests that lighter skin color evolved to optimize vitamin D production. Since vitamin D is essential in many vital functions of the body, it is argued that evolution of lighter skin color of people in higher latitudes is a genetic adaptation. At higher latitudes, lighter skin color evolved to facilitate vitamin D production under conditions of low UVB radiation in order to avoid ill health and sustain population.7
What are the Biological Functions of Vitamin D in Humans?
Vitamin D is essential for the formation of healthy bones and teeth as it helps the body to absorb, retain, and use calcium and phosphorous. 1,25(OH)2D stimulates intestinal calcium absorption.1 However, recent studies suggest many extraskeletal actions of vitamin D. The vitamin D receptor (VDR) is found in nearly all, if not all, cells in the body.8 The enzyme that produces the active metabolite of vitamin D and ligand for VDR likewise is widely expressed in many cells of the body. Vitamin D has recently been found: 1) to be protective against cancer, 2) to help keep the immune system efficient, 3) to possibly help prevent high blood pressure, 4) to play a role in the prevention of Type 2 diabetes, and 5) to maybe have a stimulating effect on specific substances in the brain, called neurotrophins, which regulate neuronal cells and their activity, and regulate cognitive function.9
Who is Susceptible to Vitamin D Deficiency?
Breast-fed infants can be susceptible to vitamin D deficiency. Vitamin D requirements cannot ordinarily be met by human milk alone.10 The American Association of Pediatricians (AAP) recommends that exclusively and partially breastfed infants must be supplemented with 400 IU of vitamin D per day. According to the United States Institute of Medicine, the recommended dietary allowances (RDA) of vitamin D for older adults are 600-800 IU/day.9 The skin of older adults cannot synthesize vitamin D as efficiently. These individuals are likely to spend more time indoors and have inadequate intakes of the vitamin. Homebound individuals, women who wear long robes and head coverings for religious reasons, and people with occupations that limit sun exposure are unlikely to obtain adequate vitamin D from sunlight. Darker skin individuals who have larger amounts of the pigment melanin in the epidermal layer may have reduced ability to produce vitamin D from sunlight. Since vitamin D is fat soluble, individuals with reduced ability to absorb dietary fat might require vitamin D supplements.9,11
Clinical Benefits of Vitamin D
Given the pivotal role vitamin D3 plays in human physiology, supplementation has been reported to benefit a variety of conditions including reduced risk of death in the elderly, improved bone health, and prevention osteoporosis.11 Vitamin D deficiency causes osteomalacia (called rickets when it occurs in children); however, supplementation of vitamin D in children with normal vitamin D levels does not appear to improve bone density. Associations have been shown in observational studies between low vitamin D levels and the risk of development of certain cancers, including colon cancer. It is unclear, however, if consuming additional vitamin D in the diet or as supplements affects the risk of cancer. Vitamin D supplementation has been proposed to reduced cardiac risk, improve immune function, reduce type 2 diabetes, ward off infections, and alleviate asthma and other auto immune diseases. However, conclusive clinical data is lacking in all these claims.9
What is the Controversy Regarding Vitamin D and Sunscreen Use?
Adequate amounts of vitamin D can be produced with moderate sun exposure to the face, arms, and legs, averaging 5-30 minutes twice per week, or approximately 25% of the time required for minimal sunburn.1 The darker the skin, and the weaker the sunlight, the more minutes of exposure are required. Vitamin D overdose is impossible from UV exposure as the skin reaches equilibrium and the vitamin degrades as fast as it is created.1 It has been suggested that people of color produce less vitamin D in response to UVB. However, this has been contested by studies that have shown that in blacks and whites sequential suberythemal UVB exposure produces similar elevation of serum 25OHD3 concentrations and unchanged 1,25(OH)2D3 concentrations.12
Sunscreen absorbs or reflects UV light and prevents much of it from reaching the skin. Sunscreen with a sun protection factor (SPF) of 8—based on the UVB spectrum—decreases vitamin D synthetic capacity by 95%, and SPF 15 decreases it by 98%.1 Recent studies suggest that short-term sunscreen use probably does not affect circulating vitamin D levels, and hence does not increase the risk for osteoporosis. Although use of a 50+ SPF sunscreen significantly decreases cutaneous vitamin D production following a single UVB exposure (independent of exposed body surface area), the circulating 25(OH)D3 levels are only minimally affected. The effect of long-term sunscreen use remains, however, to be determined.13
Is Measurement of Vitamin D in Serum an Accurate Measure of Deficiency?
It is believed that only the non-bound fraction (the free fraction) of hormones that circulate in blood is able to enter cells and exert their biologic effects. For vitamin D metabolites, less than 1% (0.4% for 1,25(OH)2D and 0.03% for 25(OH)D3) is free, with more than 99% bound to the vitamin D binding protein (DBP) and albumin (approximately 85% and 15%, respectively). Assays only measure the free vitamin D metabolite levels, and initial studies indicate their value varies in subjects with altered DBP levels. Whether the bound form of vitamin D is released as/ when needed, is not clear.14
Can Vitamin D Be Used in Cosmetics and Skin Care Products?
The hormonal form of vitamin D and its less calceotrophic analogues have been successfully used for the treatment of psoriasis.15 However, its efficacy in atopic dermatitis and eczema is disputed.16 The non-hydroxylated vitamin D that is produced in the skin does not bind to the VDR and is, therefore, ineffective for any topical clinical applications. The hydroxylated form of vitamin D (1,25(OH)2D3 and 25(OH)D3) are not allowed to be used in cosmetic products. Some cosmetic companies use precursor forms of vitamin D or vitamin D-like molecules in cosmetic products that are believed to interact with the VDR.17 However, it should be noted that their benefits have not yet been proven.
Concluding Remarks
Vitamin D3, the natural form of vitamin D, is synthesized in human skin from cholesterol precursors by the action of UV light from sunlight. The vitamin D synthesized in skin is then activated in the liver, followed by the kidneys, to the hormonally active form of vitamin D—1,25(OH)2D3. Vitamin D is not only synthesized in the skin, it also regulates skin functions including the epidermal cells and melanocytes that regulate skin pigmentation. The hormonal form of vitamin D and its analogues are used widely for the treatment of hyper-proliferative skin conditions such as psoriasis. However, they are not allowed to be used in cosmetic products. The classical role of vitamin D is in regulation of calcium and phosphorous absorption and maintenance of healthy bone. However, recent findings that vitamin D receptors are present universally in all cell types indicate a wide variety of roles in maintenance and prevention of diseases in humans. Thus, skin plays a major role in human health by producing and supplying the sunshine hormone, vitamin D, to the other organs of the human body.
References
1. M. Wacker and M.F. Holick, Sunlight and vitamin D: a global perspective for health, Dermatoendocrinol., 5, 51-108 (2013).
2. R.-J.H. Keegan, Z. Lu, J.M. Bogusz, J.E. Williams, and M.F. Holick, Photobiology of vitamin D in mushrooms and its bioavailability in humans, Dermatoendocrinol., 5, 165-176 (2013).
3. S. Pillai, D.D. Bikle, and P.M. Elias, Vitamin D and epidermal differentiation: evidence for a role of endogenously produced vitamin D metabolites in keratinocyte differentiation, Skin Pharmacol., 1, 149-160 (1988).
4. K. AlGhamdi, A. Kumar, and N. Moussa, The role of vitamin D in melanogenesis with an emphasis on vitiligo, Indian J. Dermatol. Venereol. Leprol., 79, 750-758 (2013).
5. F. Libon, J. Courtois, C. Le Goff, P. Lukas, N. Fabregat-Cabello, L. Seide, E. Cavalier, and A.F. Nikkels, Effect of body site and surface on vitamin D and 25-hydroxyvitamin D production after a single narrowband UVB exposure, J. Invest. Dermatol., 137, 1391–1393 (2017).
6. J.F. Scott, L.M. Das, S. Ahsanuddin, Y. Qiu, A.M. Binko, Z.P. Traylor, S.M. Debanne, K.D. Cooper, R. Boxer, and K.Q. Lu, Oral vitamin D rapidly attenuates inflammation from sunburn: an interventional study, J. Invest. Dermatol., 137, 2078–2086 (2017).
7. A.W. Yuen and N.G. Jablonski, Vitamin D: in the evolution of human skin colour, Med. Hypotheses, 74, 39-44 (2010)
8. Y. Wang, J. Zhu, and H.F. DeLuca, Where is the vitamin D receptor? Arch. Biochem. Biophys., 523, 123-133 (2012).
9. Vitamin D, www.wikipedia.org.
10. E. Stoutjesdijk, A. Schaafsma, N.V. Nhien, G.L. Khor, I.P. Kema, B.W. Hollis, D.A.J. Dijck-Brouwer, and F.A.J. Muskiet, Milk vitamin D in relation to the 'adequate intake' for 0-6-month-old infants: a study in lactating women with different cultural backgrounds, living at different latitudes, Br. J. Nutr., 118, 804-812 (2017).
11. R. Nair and A. Maseeh, Vitamin D: the "sunshine" vitamin, J. Pharmacol. Pharmacother., 3, 118-126 (2012).
12. W.F. Brazerol, A.J. McPhee, F. Mimouni, B.L. Specker, and R.C. Tsang, Serial ultraviolet B exposure and serum 25 hydroxyvitamin D response in young adult American blacks and whites: no racial differences, J. Am. Coll. Nutr., 7, 111-118 (1988).
13. F. Libon, J. Courtois, C. Le Goff, P. Lukas, N. Fabregat-Cabello, L. Seidel, E. Cavalier, and A.F. Nikkels, Sunscreens block cutaneous vitamin D production with only a minimal effect on circulating 25-hydroxyvitamin D, Arch. Osteoporos., 12, 66 (2017); doi: 10.1007/s11657-017-0361-0.
14. D.D. Bikle, S. Malmstroem, and J. Schwartz, Current controversies: are free vitamin metabolite levels a more accurate assessment of vitamin D status than total levels?, Endocrinol. Metab. Clin. North Am., 46, 901-918 (2017).
15. M. Oquendo, W. Abramovits, and P. Morrell, Topical vitamin D analogs available to treat psoriasis, Skinmed., 10, 356-360 (2012).
16. K. de Carvalho Mesquita, A.C. de Souza Machado Igreja, and I.M. Carvalho Costa, Atopic dermatitis and vitamin D: facts and controversies, An. Bras. Dermatol., 88, 945-953 (2013).
17. M. Yeomans, Silab launches vitamin D active for aging skin, Cosmetic Design, July 4, 2012.