
By Basma Elmogy
April 15, 2017
Stretch marks are caused by the excessive stretching of the skin that results from rapid weight gain or loss, pregnancy, and use of corticosteroids. The abdomen, breast, thighs, and buttocks are the most affected areas of the body. The medical term for stretch marks is striae distensae (usually referring to stretch marks formed due to rapid weight gain or loss) and striae gravidarum (stretch marks appearing during pregnancy). We will utilize the term striae distensae throughout the text unless referring specifically to cases of striae gravidarum.
The development of striae distensae is not a life-threatening medical condition, although, it has a profound psychological effect on the patient. The variation of the quantity and quality of the elastic fiber components in the skin has been found to correlate with the appearance of stretch marks. Therefore, most striae distensae treatments target the dermis structure. Since the fibroblast has a distinctive role in wound healing, it is suggested that treatments targeting the fibroblast should improve the condition of striae distensae by increasing the synthesis of collagen and elastin fibers in the skin.1,2 In this article, we provide an overview of striae distensae as well as some of its treatment options.
Epidemiology
The appearance of stretch marks depends on racial background as well as gender. For example, Black African women are more likely to develop striae distensae than Caucasian women living in the same geographical location.3 Furthermore, the severity of the condition is greater in Black African women. In comparison to males, the incidence of striae distensae development in females is twice as much.4 In addition, striae distensae (striae gravidarum) takes place in 90% of pregnant women, becoming very obvious in the postpartum stage.5
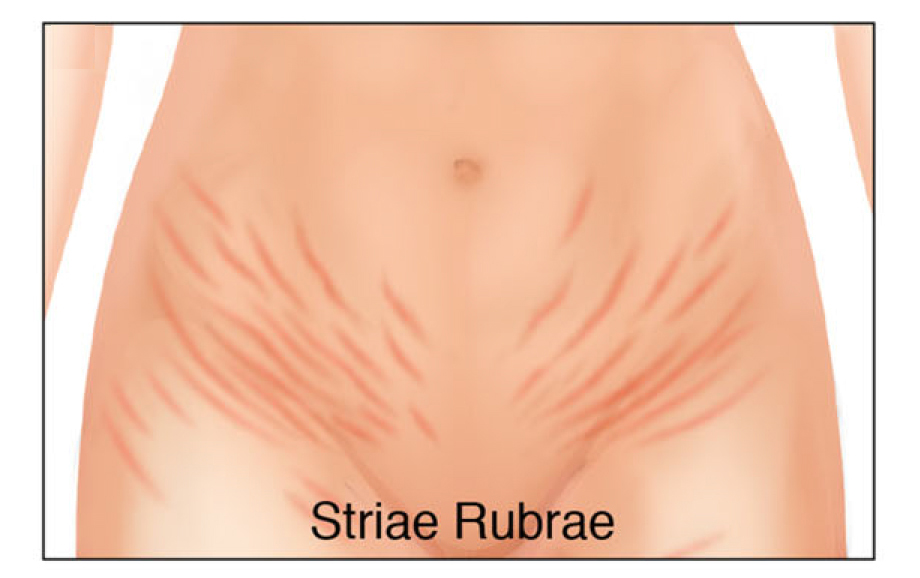
Figure 1: Illustration of striae rubrae in the abdomen region demonstrating their erythematous characteristics. Reprinted with permission according to the Creative Commons Attribution-NonCommercial-NoDerivs license from S. Ud-Din et al., Topical management of striae distensae (stretch marks): prevention and therapy of striae rubrae and albae, J. Eur. Acad. Dermatol. Venereol., 30, 211-222 (2016).
Histopathology
Striae distensae are lesions that result from stretching of the dermis. They are classified into two forms: 1) the early stage (striae rubrae), which is characterized by erythema and stretch marks that are perpendicular to the direction of skin tension and 2) the later stage (striae albae), which is reminiscent of scarring and has an atrophic, wrinkled, and hypopigmented appearance.6,7 Early stages (striae rubrae) show superficial and deep perivascular infiltrates of lymphocytes and eosinophils, in addition to dilation of venules and swelling in the upper part of the dermis, which is associated with erythema. Mature lesions (striae albae), on the other hand, have a thin infiltrate of lymphocytes. Striae albae are further characterized by flattening and thinning of the skin. In addition, dermal papilla begin to disappear and are replaced by collagen bundles, and hair follicles and other appendages vanish at this point.1,8
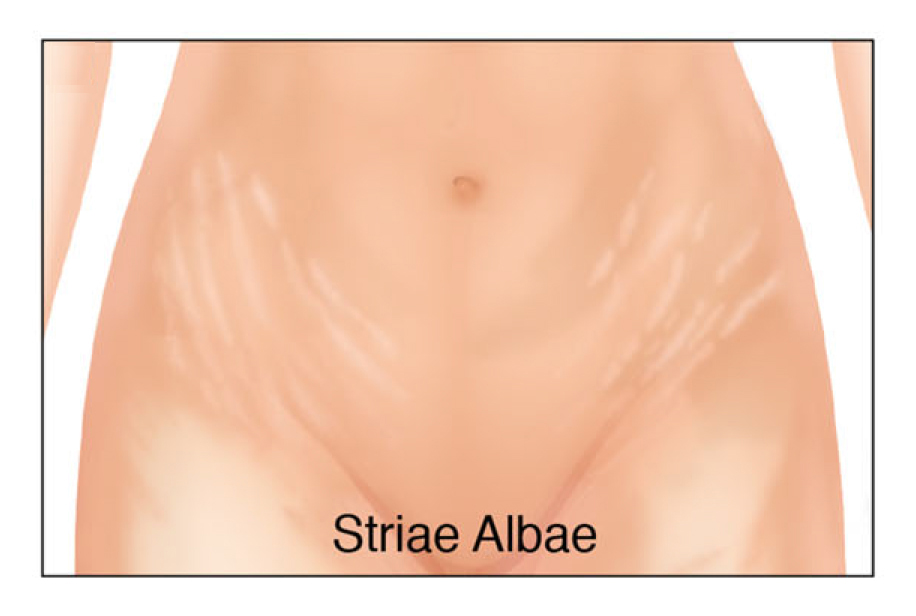
Figure 2: Illustration of striae albae in the abdomen region demonstrating their atrophic, hypopigmented characteristics. Reprinted with permission according to the Creative Commons Attribution-NonCommercial-NoDerivs license from S. Ud-Din et al., Topical management of striae distensae (stretch marks): prevention and therapy of striae rubrae and albae, J. Eur. Acad. Dermatol. Venereol., 30, 211-222 (2016).
Etiology
The cause of striae distensae is still not entirely clear. Some authors have pointed out that stretch marks are a form of stress rupture of the connective tissue network.1 Some genetic factors lead to a decrease in the elastic fiber network and affect its organization with fibrillin. Interestingly, striae distensae are associated with depletion in the expression of collagens, elastin, and fibronectin genes.9 Furthermore, the absence of cross-linking (e.g., within the collagen network) provides the skin with the ability to undergo more stretching.4
Systemic and local treatment with glucocorticoid drugs may also cause dermal atrophy.8 Studies also emphasize that there is a link between glucose intolerance and the appearance of striae distenae. In addition, researchers propose that the formation of stretch marks is connected to adrenal cortical activity. As a result, the expression of estrogen, androgen, and glucocorticoid receptors is elevated in regions of the skin that undergo mechanical stretching.10
In pregnancy, the intensified stretching of the skin leads to transformation and disturbance in the extracellular matrix, which causes remodelling of the fibrillin components in the elastic fiber network and allows the skin to be easily torn.8 In essence, this is dermal scarring. The elevation of steroid levels in the blood, hormonal changes, and disturbance in glucose levels during pregnancy, all contribute to the formation of striae distensae.1 Furthermore, estrogen, relaxin, and corticosteroids are thought to encourage the synthesis of certain types of mucopolysaccharides which boost detachment of the collagen fibrils causing stretch marks.11
Treatment
The options for treating striae distensae are topical agents as well as laser treatments or light therapy. There are numerous studies in the literature that focus on a variety of different topical treatments. Retinoic acid, or tretinoin, has probably received the most attention due to its important role in the treatment of compromised (e.g., photoaged skin or acne afflicted skin), and in some cases, scarred skin. In addition, many efforts have been made to investigate the effect of other topicals including centella (a medicinal herb), hyaluronic acid, cocoa butter, olive oil, and almond oil.12
Overall, retinoic acid shows promise of partial reduction of striae distensae if treatment is administered in the early stages (striae rubrae).7 The exact mechanism of how retinoic acid works is not fully understood; however, its ability to restore collagen levels in photodamaged skin is believed to play an important role. In addition, retinoic acid modulates keratinocyte proliferation and differentiation in the epidermis, which could result in an alteration of keratinocyte cytokine expression and may induce the synthesis of collagen or reduce collagenase activity. This is justified by the example of transforming growth factor beta, which is induced in the keratinocyte by retinoic acid treatment and in turn influences collagen biosynthesis by the fibroblast.
Combination therapies have also sparked interest in the research community to increase the efficacy of retinoic acid treatment. For example, one approach is to supplement retinoic acid treatment with alpha hydroxy acids, such as glycolic acid.13 Another strategy includes the use of fractional radiofrequency with acoustic pressure ultrasound to deliver retinoic acid transepidermally to enhance its effect on the stretch marks.14
Among the other topical treatments, there is some evidence, although weak, that almond oil, hyaluronic acid, and centella provide benefits to skin afflicted by striae distenae. Treatment with cocoa butter (sometimes combined with vitamin E) and olive oil are not effective agents at preventing or reducing striae distensae.12
As already mentioned, laser techniques and light therapy are also viable options to treat striae distensae.15,16 Laser techniques consist of ablative, nonablative, and fractional resurfacing. Out of the three protocols, non-ablative laser techniques have been investigated the most for treating striae distensae. They operate by irradiating the skin with laser light and targeting melanin and hemoglobin. In addition to interacting with vascular chromophores (e.g., those found in striae rubrae), nonablative lasers can stimulate collagen and elastin synthesis.16 These procedures have had notable success in treating striae distensae; however, one should bear in mind that blind experiments and controls are usually not incorporated in most studies of this type.7
Concluding Remarks
Topical agents alone are not sufficient to treat striae distensae. However, if administered in the early stages, retinoic acid is a promising treatment for alleviating the degree of severity of the condition. Moreover, retinoic acid may be combined with other treatment modalities, such as alpha-hydroxy acids or light therapy. Nonablative laser therapy is also an encouraging option that has shown promise to reduce striae distensae.
References
1. M.L. Elson, Topical tretinoin in the treatment of striae distensae and in the promotion of wound healing: A review, J. Dermatol. Treat., 5, 163-165 (1994).
2. J.Á. García Hernández, D. Madera González, M. Padilla Castillo, and T. Figueras Falcón, Use of a specific anti-stretch mark cream for preventing or reducing the severity of striae gravidarum. Randomized, double-blind, controlled trial, Int. J. Cosmet. Sci., 35, 233-237 (2013).
3. N. Elbuluk, S. Kang, and T. Hamilton, Differences in clinical features and risk factors for striae distensae in African American and white women, J. Am. Acad. Dermatol., 60 Supp. 1, AB56 (2009).
4. D.S. Sarnoff, Therapeutic update on the treatment of striae distensae, J. Drugs Dermatol., 14, 11-12 (2015).
5. O. Rangel, I. Arias, E. García, and S. Lopez-Padilla, Topical tretinoin 0.1% for pregnancy-related abdominal striae: an open-label, multicenter, prospective study, Adv. Ther., 18, 181-186 (2001).
6. S. Ud-Din, D. McGeorge, and A. Bayat, Topical management of striae distensae (stretch marks): prevention and therapy of striae rubrae and albae, J. Eur. Acad. Dermatol. Venereol., 30, 211-222 (2016).
7. S. Al-Himdani, S. Ud-Din, S. Gilmore, and A. Bayat, Striae distensae: a comprehensive review and evidence-based evaluation of prophylaxis and treatment, Br. J. Dermatol., 170, 527-547 (2014).
8. G. El-Khalafawy, Comparative study between intense pulsed light “IPL” and pulsed dye laser in the treatment of striae distensae, Ph.D. dissertation, National Institute of Laser Enhanced Sciences, Cairo University, Cairo, Egypt (2013).
9. K.S. Lee, Y.J. Rho, S.I. Jang, M.H. Suh, and J.Y. Song, Decreased expression of collagen and fibronectin genes in striae distensae tissue, Clin. Exp. Dermatol., 19, 285-288 (1994).
10. R.C. Cordeiro, K.G. Zecchin, and A.M. de Moraes, Expression of estrogen, androgen, and glucocorticoid receptors in recent striae distensae, Int. J. Dermatol., 49, 30-32 (2010).
11. M. Brennan, G. Young, and D. Devane, Topical preparations for preventing stretch marks in pregnancy, Cochrane Database Syst. Rev., November 14, 11:CD000066 (2012).
12. K. Korgavkar and F. Wang, Stretch marks during pregnancy: a review of topical prevention, Br. J. Dermatol., 172, 606-615 (2015).
13. K. Ash, J. Lord, M. Zukowski, and D.H. McDaniel, Comparison of topical therapy for striae alba (20% glycolic acid/0.05% tretinoin versus 20% glycolic acid/10% L-ascorbic acid), Dermatol. Surg., 24, 849-856 (1998).
14. M.C. Issa, L.E. de Britto Pereira Kassuga, N.S. Chevrand, L. do Nascimento Barbosa, R.R. Luiz, L. Pantaleão, E.G. Vilar, and M.C. Rochael, Transepidermal retinoic acid delivery using ablative fractional radiofrequency associated with acoustic pressure ultrasound for stretch marks treatment, Lasers Surg. Med., 45, 81-88 (2013).
15. J.A. Savas, J.A. Ledon, K. Franca, and K. Nouri, Lasers and lights for the treatment of striae distensae, Lasers Med. Sci., 29, 1735-1743 (2014).
16. A.S. Aldahan, V.V. Shah, S. Mlacker, S. Samarkandy, M. Alsaidan, and K. Nouri, Laser and light treatments for striae distensae: A comprehensive review of the literature, Am. J. Clin. Dermatol., 17, 239-256 (2016).